
Shoulder Introduction
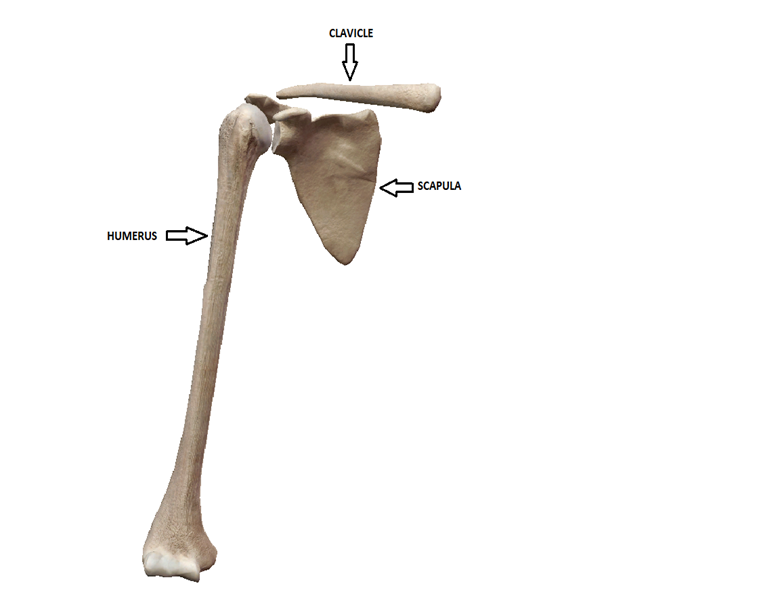
The shoulder is one of the largest, most flexible and complex joints in the body. It consists of three main bones: the humerus, scapula, and clavicle and four joints. A shoulder allows for raising, bending and rotating the arms. It is one of the most mobile joints in the entire body.
Joint
A joint is where two or more bones meet and move (articulate) on one another. The main articulations of the shoulder are between the scapula and humerus (glenohumeral joint), the scapula and clavicle (acromioclavicular joint), sternum and clavicle (sternoclavicular joint), and last the scapula and thoracic spine/ribs (scapulothoracic joint). In the synovial joints (glenohumeral, acromioclavicular, and sternoclavicular) the articulating surfaces of the bones are covered with a layer of hyaline cartilage also called articular cartilage. This cartilage provides a smooth almost frictionless surface for the bones to move on one another. The scapulothoracic joint is a muscular articulation between the scapular and thoracic area.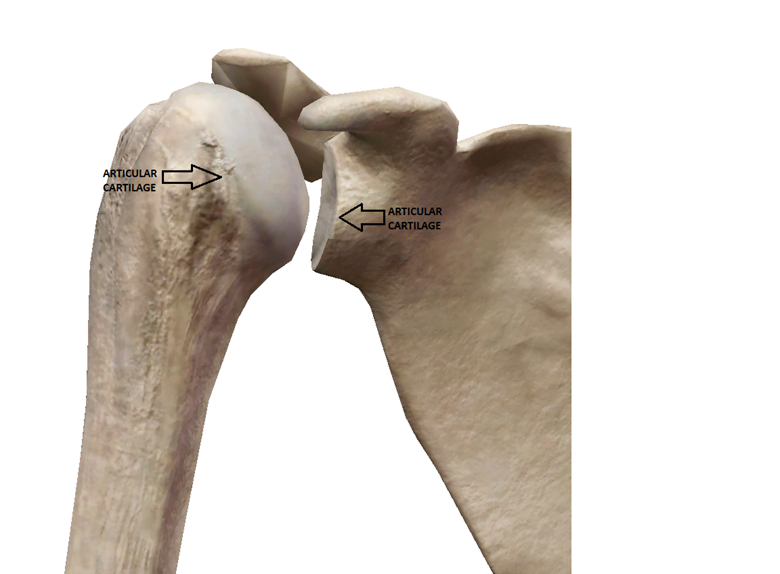
Glenohumeral joint
The glenohumeral joint of the shoulder is a ball and socket joint formed by the proximal end of the humerus and glenoid fossa of the scapula (shoulder blade).
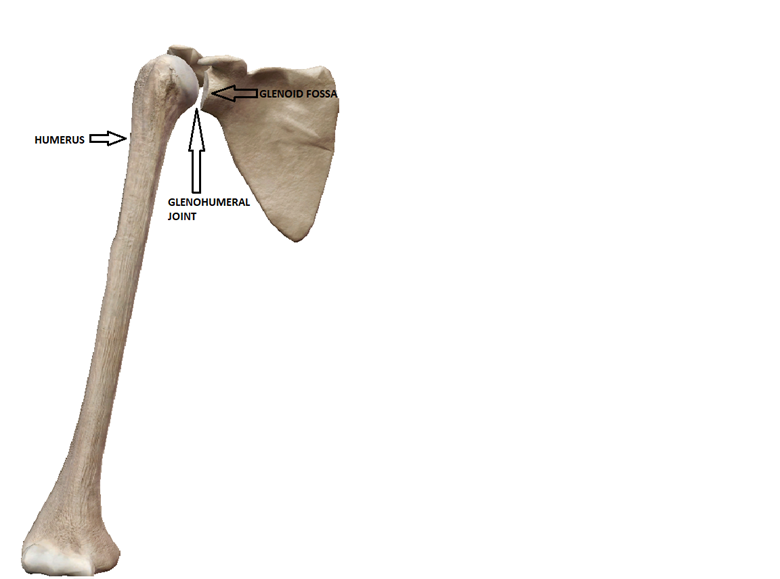
The main motions of this joint are flexion and extension, abduction and adduction, horizontal abduction and adduction, external rotation and internal rotation, and circumduction. The glenohumeral joint can also move in diagonals which are combined motions through the cardinal planes.

Acromioclavicular joint (AC JOINT)
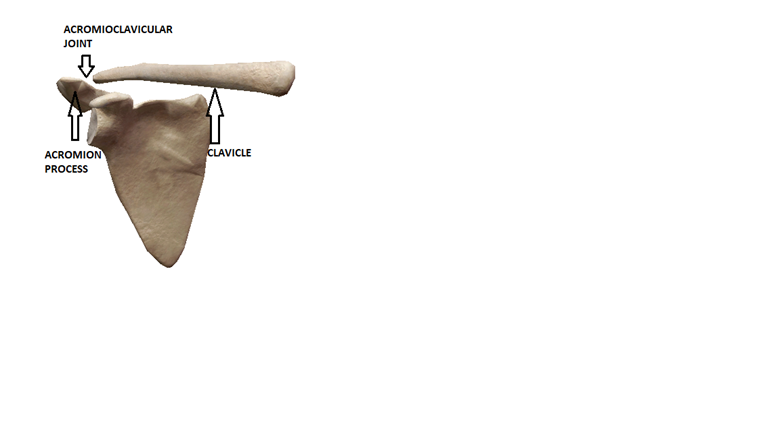
The Acromioclavicular joint (AC JOINT) of the shoulder is formed by the acromion of the scapula and the distal end of the clavicle (collar bone). The AC joint along with the sternoclavicular joint and scapulothoracic joint allow for the motions: scapular protraction and retraction, scapular elevation and depression, scapular upward and downward rotation.
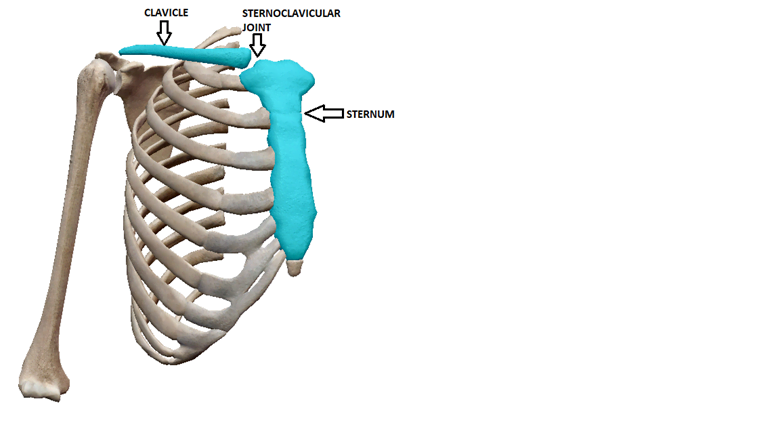
Sternoclavicular joint (SC JOINT)
The Sternoclavicular joint (SC JOINT) of the shoulder is formed by the superior/lateral aspect of the sternum and the proximal end of the clavicle (collar bone). The SC joint along with the AC joint and scapulothoracic joint allow for the motions: scapular protraction and retraction, scapular elevation and depression, scapular upward and downward rotation.
Scapulothoracic joint
The Scapulothoracic joint of the shoulder is formed by the scapula and its muscular attachments to the thoracic spine/ribs. The scapulothoracic joint along with the AC joint and SC joint allow for the motions: scapular protraction and retraction, scapular elevation and depression, scapular upward and downward rotation.


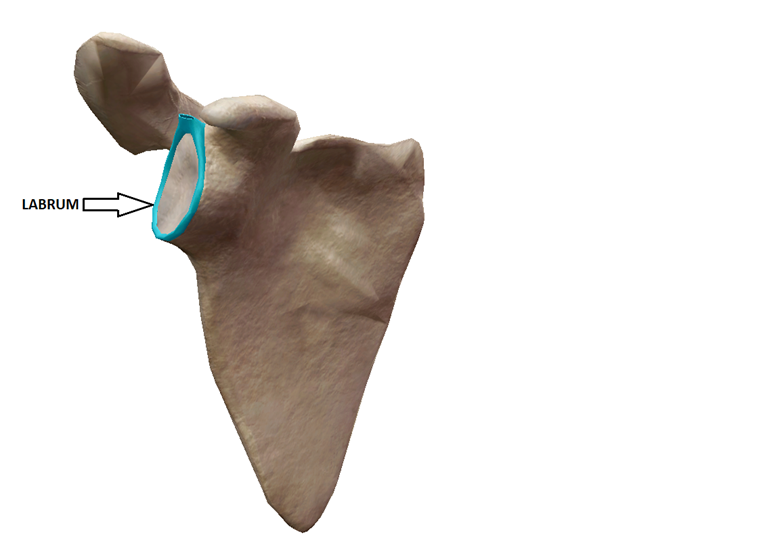
Labrum
The scapula has a rubbery fibrocartilage structure that wraps around and attaches to the rim of the glenoid fossa. The labrum is thicker at the periphery and thinner at the inside edges making a cup shape. The labrum deepens the articular surface of the glenoid to increase joint congruency and stabilizes the large head of the humerus.
Ligaments
Ligaments are fibrous connective tissue that attach bone to bone. They promote proper joint mechanics, as well as prevent excessive joint movement. Below are the major ligaments of the shoulder complex.
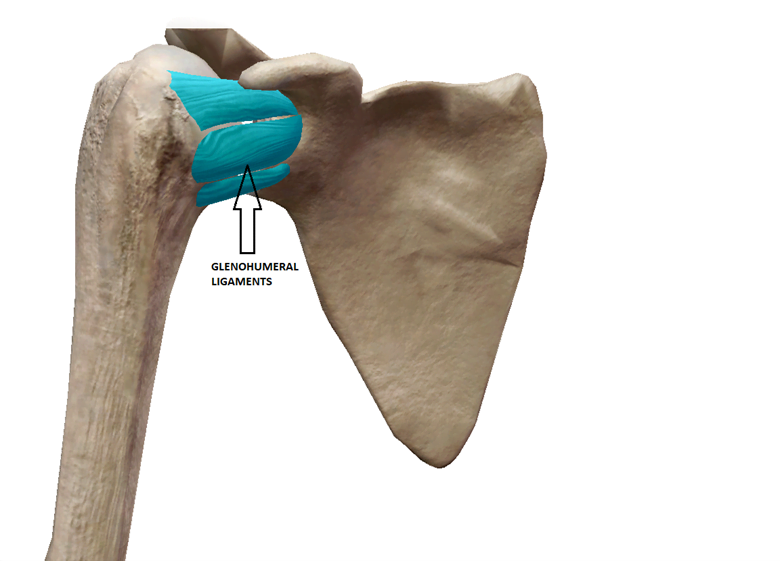
Glenohumeral(GH) ligaments
The glenohumeral ligaments attach from the outside rim of the glenoid to the humerus. The ligaments include: the superior, medial, and inferior GH ligament. These ligaments prevent humeral dislocation.
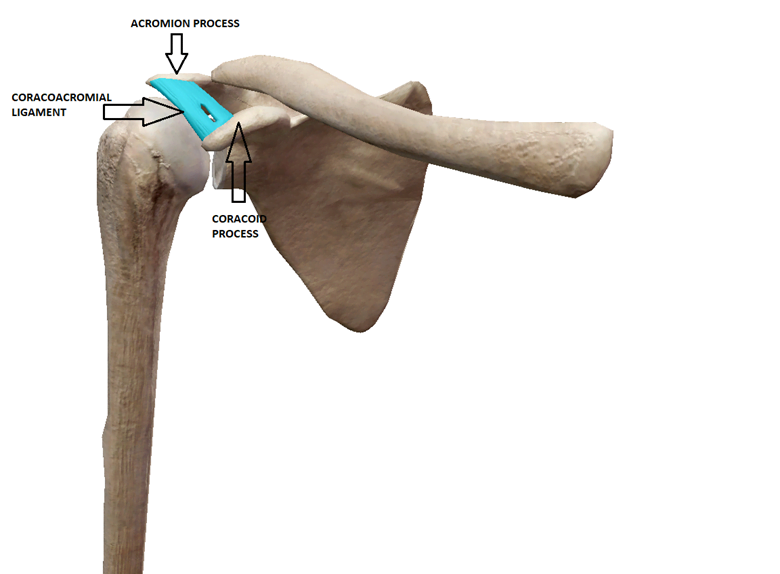
Coracoacromial ligament
The coracoacromial ligament attaches from the coracoid process to the acromion of the scapula and makes a roof over the shoulder joint to prevent superior dislocation.
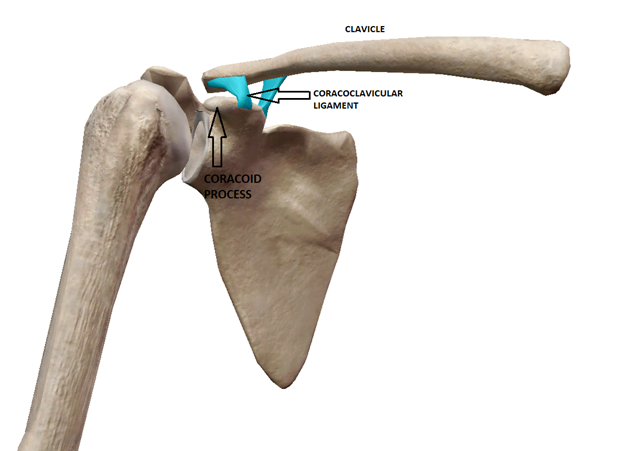
Coracoclavicular ligament
The coracoclavicular ligament is made up of the conoid and trapezoid ligament which attach from the coracoid process to the clavicle. The ligaments prevent dislocation of the clavicle.
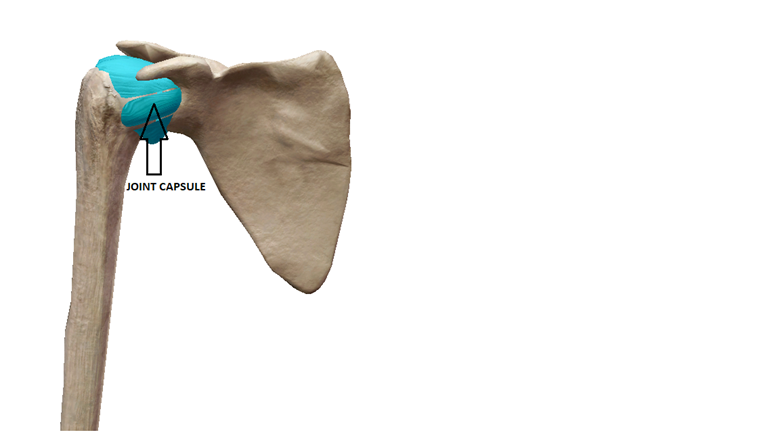
Joint capsule
The joint capsule is a fluid filled layer of fibrous connective tissue that surrounds the entire joint and encapsulates it. The joint capsule provides joint stability, proprioception, and prevents excessive movement in all directions. It is also essential for joint nutrition and lubrication as the inside layer of the capsule has a synovial membrane that secretes synovial fluid.
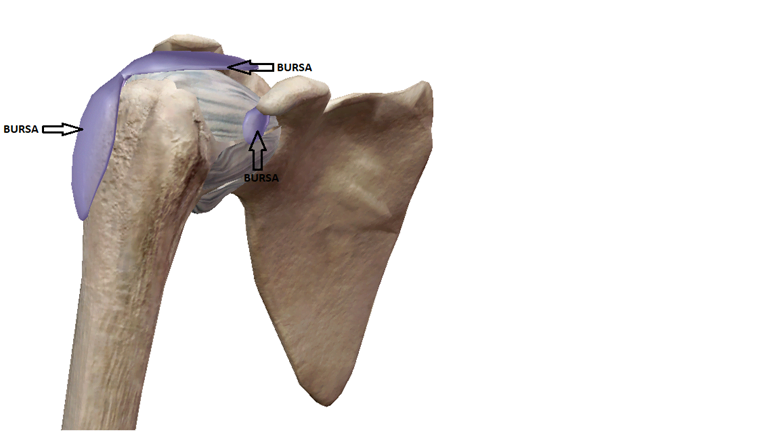
Bursae are small fluid-filled sacs that rest in between moving parts near joints and reduce friction thus preventing tissue wearing. Below are a major bursae of the shuolder:
-Subacromial bursa
-Subdeltoid bursa
-Subcoricoid bursa
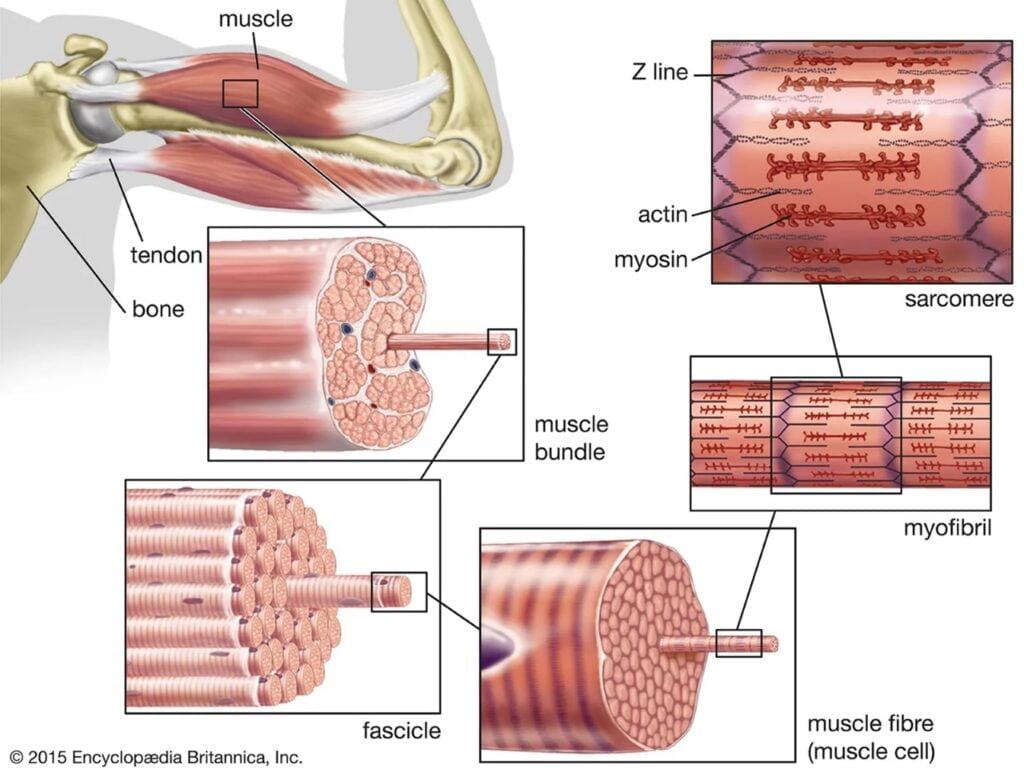
Muscle(s) and Tendon(s)
Skeletal muscle is made of bundles of contractile fibers that produce movement. The muscle attaches to bone via a tendon which is made of fibrous connective tissue. All skeletal muscles have a proximal and distal tendon, and when the muscle contracts/shortens it pulls the attached bones closer together. Muscles not only produce bodily movement, but also control movement and stabilize joint(s) and posture(s). Below are some of the important muscles and tendons of the shoulder:
Rotator cuff
The rotator cuff is a group of four muscles (supraspinatus, infraspinatus, teres minor, subscapularis) that attach from the scapula to the humerus. The rotator cuff is important for proper shoulder function as they stabilize the humeral head in the glenoid socket.
BACK VIEW

FRONT VIEW
Supraspinatus
The supraspinatus attaches from the supraspinous fossa to the greater tuberosity of the humerus. It functions to abduct the arm, as well as stabilize the glenohumeral joint.

Infraspinatus
The infraspinatus attaches from the infraspinous fossa to the greater tuberosity of the humerus. It functions to externally rotate the arm, as well as stabilize the glenohumeral joint.

Teres minor
The teres minor attaches from the lateral border to the scapula to the greater tuberosity. It functions to externally rotate the arm, as well as stabilize the glenohumeral joint.

Subscapularis
The subscapularis attaches from the subscapular fossa on the front of the scapula to the lesser tuberosity. It functions to externally rotate the arm, as well as stabilize the glenohumeral joint.

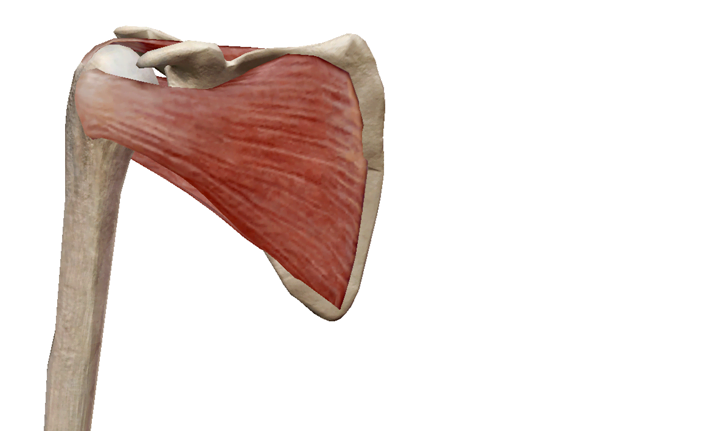
Deltoid
The deltoid is a large triangular muscle that attaches from the scapula and clavicle to the humerus. The function of the deltoid is flexion, abduction, extension, and internal/external rotation of the arm.

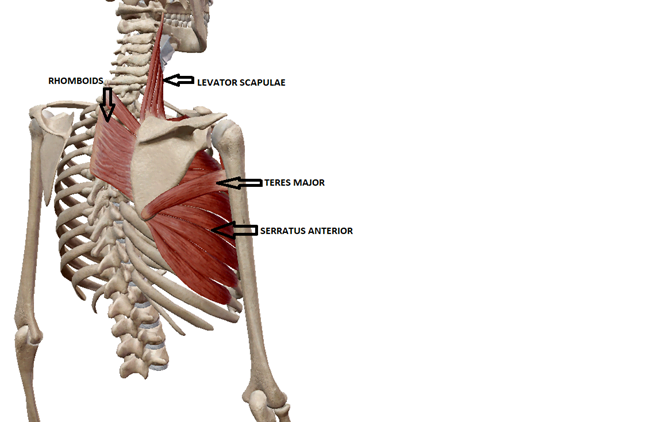
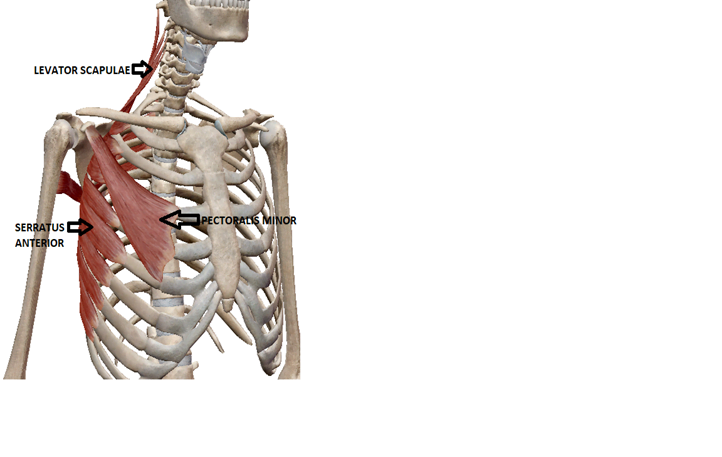
Periscapular muscles
The periscapular muscles include the trapezius, rhomboids, levator scapula, teres major, serratus anterior, and pectoralis minor. The periscapular muscles function to produce scapular movements such as elevation, depression, retraction, protraction, upward rotation, and downward rotation.

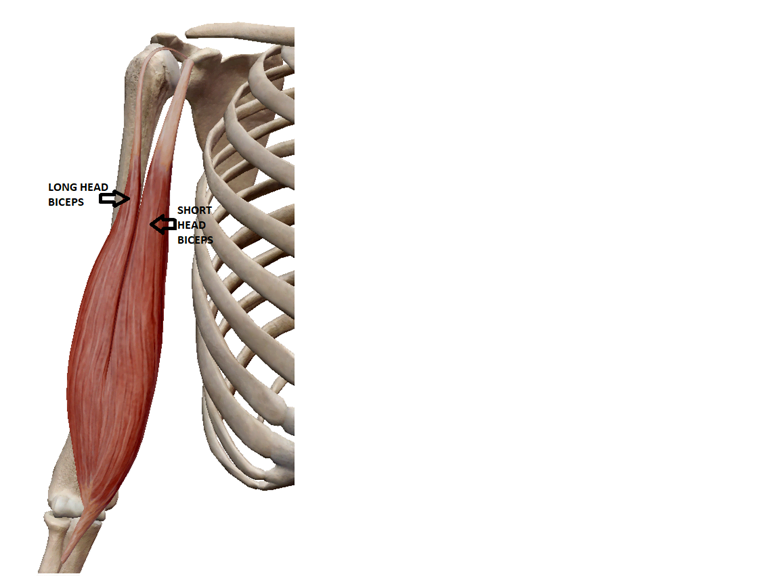
Biceps brachii
The biceps brachii have two heads: the short head and long head. The function of the biceps is not only elbow flexion, but also shoulder flexion especially when the arm is externally rotated.



0 Comments